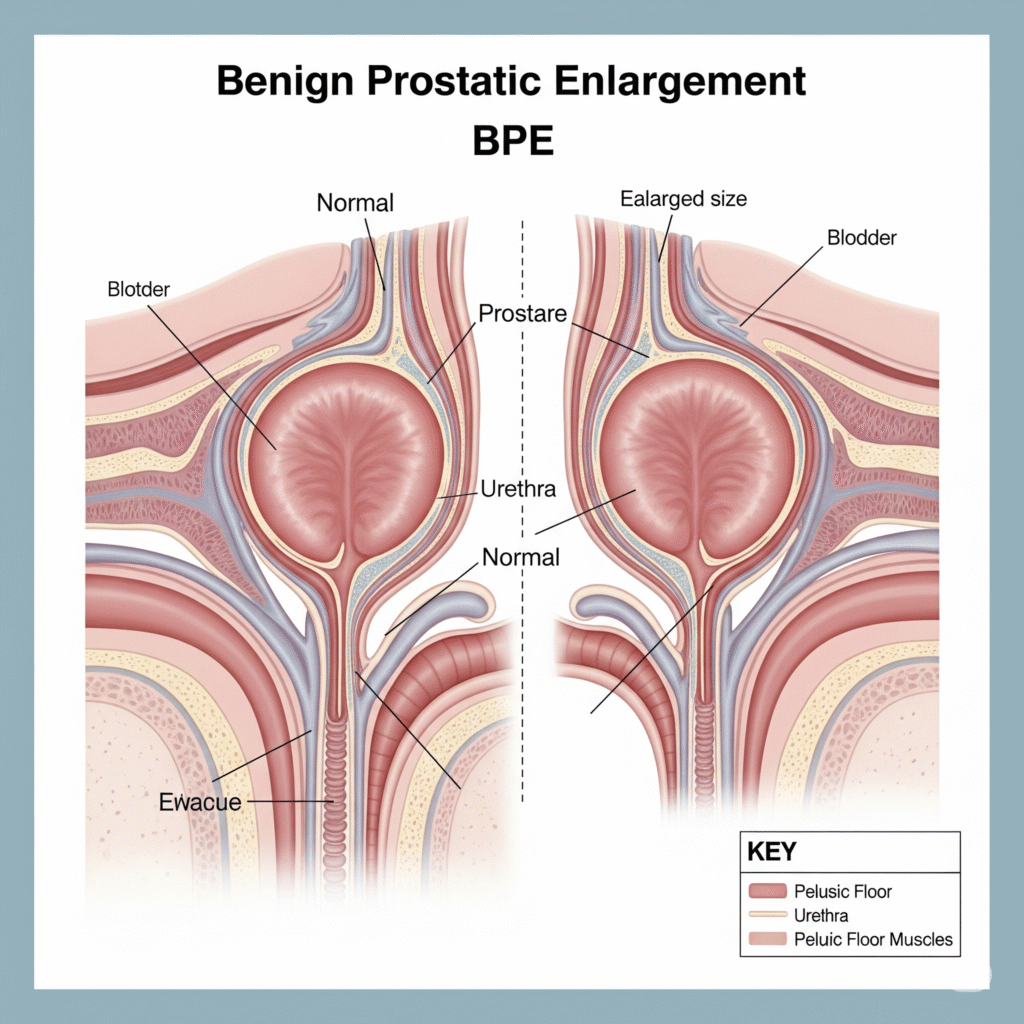
Mental prostatic enlargement (BPE) is a very common condition, especially in old men. It is estimated that about 50% of men aged and above are due to the experience of low urinary tract symptoms (LUTs) due to the outlet obstruction (BOO) of the bladder due to BPE. The underlying histological change responsible for the BPE is benign prostatic hyperplasia (BPH).
1. The most common type.
2. The extending of the right and left side side of the prostate involves the expansion of the right and left side.
3. From both sides leads to compression of the urethra, causing urinary obstruction.
1. All lobes of prostate (lateral, mean and anterior) are increased.
2. Important low urinary tract symptoms can be caused by severe urethra compression.
1. A lobe (usually a lateral one) increases more than the other.
2. Still can lead to important symptoms depending on the degree of urethra compression.
1. Histological evidence of BPH without significant increase in prostate volume or symptoms.
2. Often other reasons show the combination of imaging or during surgery.
such as hesitant, weak urine stream, and a sense of imperfect bladder emptying are common.
such as urinary frequency, urgency and urge incontinence can also occur, but are not specific to BPE.
can suddenly introduce, often begins with alcohol, constipation, or infection, causing a painful, deformed bladder.
can gradually develop and lead to kidney problems such as hydronephrosis and kidney failure.
is used to assess the severity of symptoms and involves a quality-life question.
Doubt Delay or difficulty in starting the flow of urine, often requires additional effort to start urination.
Uroflowmetry (flow meter) is used to measure urine flow rate and assess obstruction severity.
Measured using ultrasound to determine how much urine remains in the bladder after voiding.
Assessed through Transrectal Ultrasound (TRUS) to evaluate the size of the prostate gland.
Used when symptoms are unclear or mixed (both voiding and storage symptoms present), or when:
Voided volume is <150 ml, or
Flow rate is >10 mL/s but obstruction is still suspected.
Should be checked if any of the following are present:
Palpable bladder
Nocturnal enuresis (involuntary urination during sleep)
Recurrent urinary tract infections (UTIs)
History of renal stones
If renal function is found to be abnormal, ultrasound imaging should be used to look for signs of urinary tract obstruction.
Copyright © 2025 – Designed by Camsol Advertising