Chronic obstructive pulmonary disease (COPD) is a progressive lung condition that features frequent airflow boundaries and difficulties of breathing. This is usually caused by prolonged contact for cigarette smoke, dust, or irritability such as environmental pollutants. COPD contains a group of lung diseases that cause inflammation, structural damage and narrowness of airways, causing hard for air for air inside and out of the lungs.
Defined by chronic producers coughing at least three months in two consecutive years, due to inflammation of the airways and excessive mucus production.
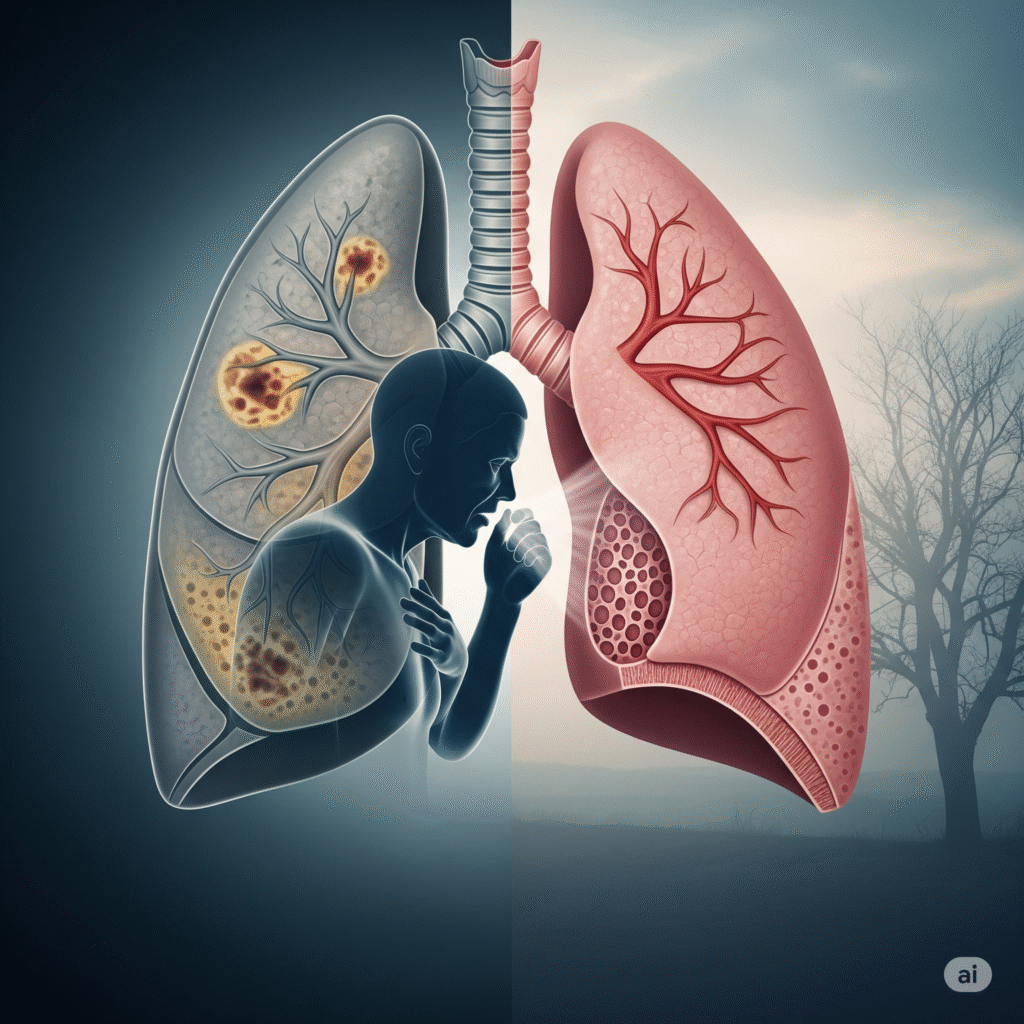
The destruction of the alveolar walls is involved, causing loss of lung elasticity and reduces the surface area for gas exchange, resulting in breath withdrawal.
A severe form of asthma that does not react well to standard drugs, causing a frequent airflow range similar to COPD.
Permanent spread of bronchi and damage, mucus accumulation and frequent respiratory infection due to frequent infection or inflammation.
Often the earliest symptoms, it may be drought or produce mucus, usually worse in the morning and continuously for years.
Chronic inflammation in the airways and thick mucus often coughs due to overdom active mucus glands.
Gradually deteriorates over time, during the first hard work and after resting, due to the airflow range and reducing the elasticity of the lungs.
A whistle or scream sound during breathing due to compressed and inflamed airways.
Constant fatigue is because the body works hard to breathe and the tissues decrease oxygen delivery.
Cyneosis, a blue color of lips or fingers due to low oxygen levels.
Hyperinflated identifies the lungs, excluding other causes of symptoms such as pneumonia or heart disease.
Provides elaborate lung images to detect emphysema, airways change, or not visible on standard X-rays.
The gas exchange evaluates the level of oxygen and carbon dioxide in the blood to assess the severity of respiratory failure.
The non-invasive method to measure oxygen saturation is useful for ongoing monitoring of oxygen levels.
Bacteria analyzes mucus for infections or abnormal cells, especially during exercise.
Cronic detect heart stress or core pulmonary (right -sided heart problems) for lung disease.
Screen for genetic deficiency that increases sensitivity to early starting emphysema.
Assesses the patient’s ability to perform physical activity and determine oxygen requirements during diligence.
Copyright © 2025 – Designed by Camsol Advertising