Renal stone disease is a widespread condition that affects individuals across all countries and ethnic backgrounds. In the United Kingdom, around 1.2% of the population is affected, with men facing an estimated 7% lifetime risk of developing a kidney stone by the age of 60 to 70. However, the risk is significantly higher in certain regions, such as Saudi Arabia, where more than 20% of men in the same age group are likely to experience renal stones during their lifetime.
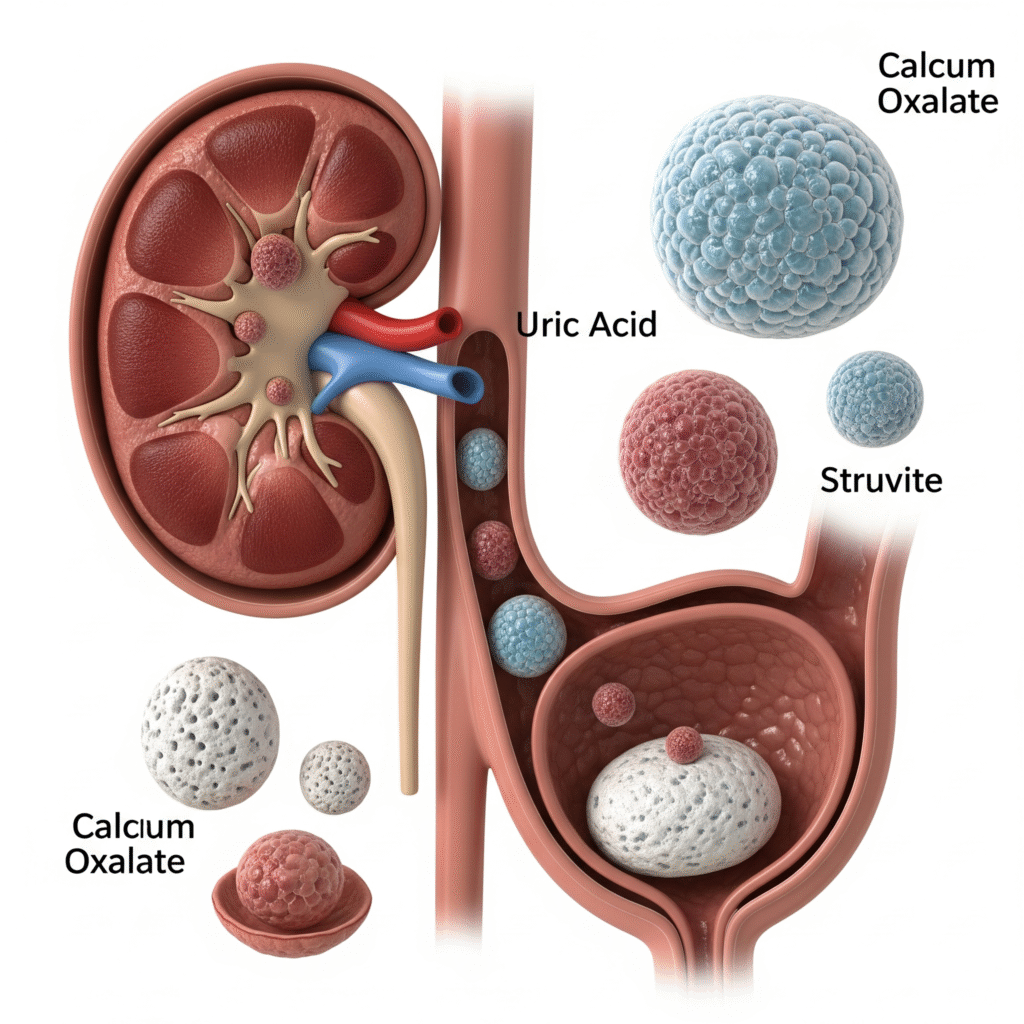
Most common type; includes calcium oxalate and calcium phosphate stones. Often linked to dehydration and high-oxalate foods.
Form in acidic urine; associated with high-protein diets, gout, and low fluid intake.
Infection-related stones caused by bacteria that produce urease; can form large staghorn calculi.
Rare stones due to a genetic disorder (cystinuria); occur when excess cystine is excreted in urine.
Sudden, sharp pain in the back or side, usually on one side.
Pain may move to the lower abdomen or groin as the stone travels
Especially if the stone is near the bladder.
You may feel like urinating often but pass only small amounts.
Similar to a urinary tract infection.
Indicates the stone is in the lower urinary tract.
Often occurs due to intense pain or blockage affecting kidney function.
Can be accompanied by sweating and restlessness.
Sharp pain in the side or back
It is important to find out where exactly the stone is located and whether it is causing any blockage to the flow of urine.
About 90% of stones contain calcium and are visible on a simple X-ray. This test is useful for detecting radio-opaque stones.
This is the gold standard investigation, as it can detect about 99% of stones in the kidney or ureter. It gives a clear image without using contrast.
Ultrasound can detect stones in the kidney and signs of blockage like swelling (hydronephrosis). It is especially helpful for pregnant women or those who should avoid radiation.
A minimum set of tests like urine analysis, serum creatinine, and blood tests should be done for every patient presenting with a first-time stone.
Detailed investigations (e.g., 24-hour urine collection) are usually reserved for patients at high risk of recurrence, such as those with recurrent stones or a family history.
If the stone is passed or removed, it should be sent for chemical analysis to identify its composition and help determine the cause.
After a renal colic episode, patients should filter their urine using a strainer for a few days to catch and collect the stone for lab testing.
Copyright © 2025 – Designed by Camsol Advertising